Pediatric CPR OSCE 2026 Update: New Zealand Guidelines on Compression Ratios, AED Pad Placement, and Clinical Sequence
The CPR station has changed — and the details matter. Here is everything you need to get it right on exam day, aligned with current New Zealand pediatric resuscitation standards.
If you have been practising CPR on children only, your preparation is incomplete. The OSCE CPR station has been updated to include a full pediatric approach — covering both children and infants. New Zealand Simulation Centre NZSC have already updated their training scenarios to match.
This guide breaks down every change: the compression-to-ventilation ratios, AED pad placement for small bodies, and the post-shock clinical sequence. Bookmark it. Drill it. Know it cold
New Zealand Pediatric Resuscitation Guidelines
All OSCE candidates are assessed against New Zealand pediatric resuscitation guidelines. This is not a minor update — the full algorithm, including age-specific ratios and pad placement for small children and infants, is now examinable.
NZSC training stations reflect the current standard, meaning your practice environment and your exam environment are aligned. There is no excuse for a guidelines mismatch on the day.
ⓘ
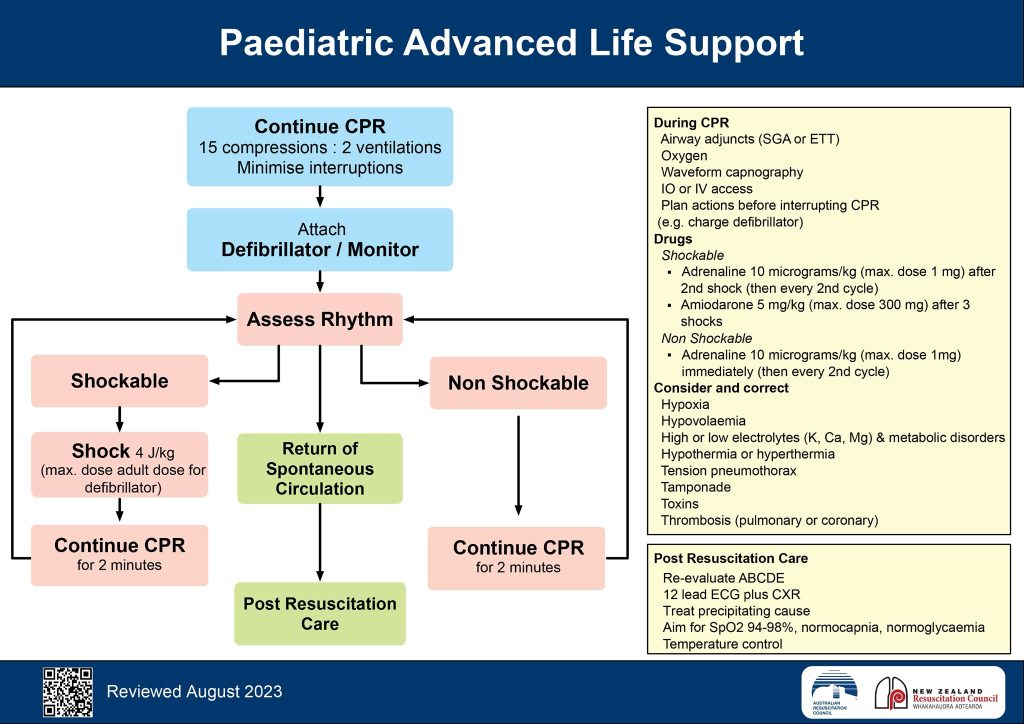
CPR Compression-to-Ventilation Ratios
The single most common critical error in the CPR OSCE station is applying the wrong compression-to-ventilation ratio for the number of rescuers in the scenario. Examiners set the scene deliberately — read it, then set your ratio.
Single rescuer 30:2 compressions : ventilations
Two rescuers 15:2 compressions : ventilations
Why does the ratio change with two rescuers?
With a single rescuer, minimising interruptions to compressions takes priority — hence the 30:2 ratio used in adult CPR as well. With two rescuers, one can manage the airway continuously while the other compresses, allowing a more frequent ventilation schedule without prolonged pauses. In pediatric patients — who are more likely to have respiratory-driven cardiac arrest — maintaining oxygenation is especially important, which is why the two-rescuer ratio shifts to 15:2.
AED Pad Placement for Small Children and Infants
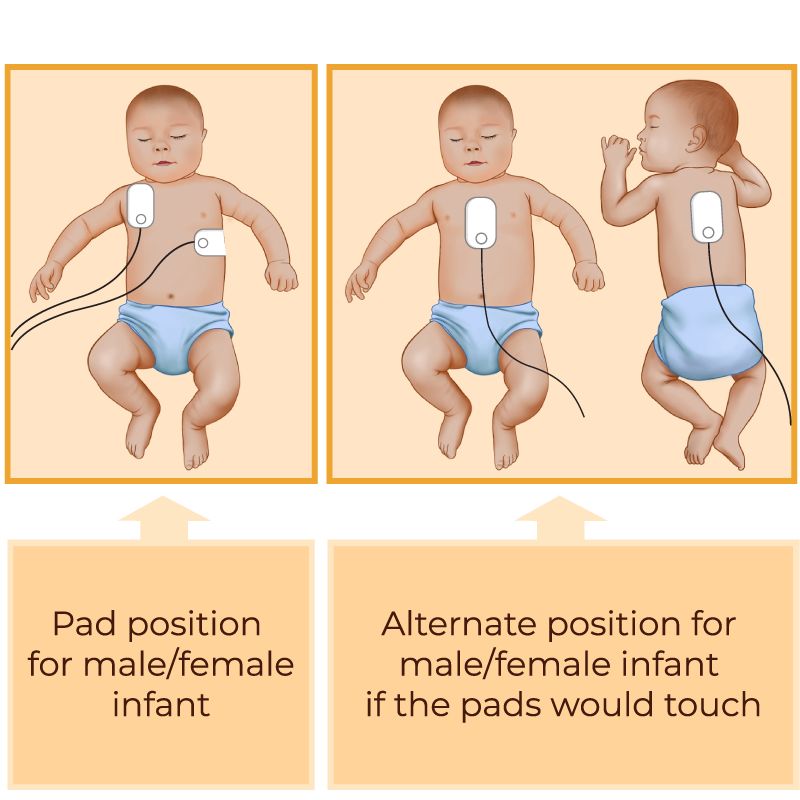
When paediatric pads are unavailable and adult pads must be used, placement technique becomes critical. On a small child or infant, the standard anterior-lateral chest placement used in adults risks the pads overlapping — and overlapping pads prevent effective shock delivery.
The correct approach is anterior-posterior placement.
Anterior-posterior placement — step by step
- 1Place one pad on the front of the chest (anterior — centre of the sternum)
- 2Place the second pad on the back, between the shoulder blades (posterior)
- 3Confirm the pads are not touching or overlapping
- 4Proceed with rhythm assessment and shock if indicated
This placement ensures the electrical vector passes directly through the myocardium, maximising the probability of successful defibrillation. With adult-sized pads on a small chest, anterior-posterior placement is the only configuration that reliably avoids pad contact and achieves adequate current density through the heart.
The Correct Clinical Sequence
Beyond the ratio and the pads, your overall sequence must be sharp. Hesitation between steps or incorrect ordering will cost you marks even if the individual actions are correct.
- 1Attach the defibrillator early — do not delay rhythm assessment waiting to complete CPR cycles
- 2Assess the rhythm — is it shockable (VF / pulseless VT)?
- 3If shockable: confirm pad placement, clear the patient, deliver the shock
- 4Resume CPR immediately after shock delivery — do not pause to recheck rhythm
- 5Continue CPR for 2 minutes before reassessing rhythm and pulse
Key Takeaways for OSCE Day
Read the scenario: single rescuer = 30:2, two rescuers = 15:2. For small children and infants with adult pads, use anterior-posterior placement — one pad on the front of the chest, one between the shoulder blades, never overlapping. Attach the defibrillator early, shock if indicated, then resume CPR immediately for 2 full minutes before reassessment. These are the three points examiners are marking.
Pediatric CPR OSCE — Common Questions
What is the correct CPR ratio for a child with two rescuers in NZ?
With two rescuers, the correct compression-to-ventilation ratio for a child or infant is 15:2 under New Zealand pediatric resuscitation guidelines. With a single rescuer, the ratio is 30:2 — the same as adult CPR — to minimise interruptions to chest compressions.
Where do you place AED pads on an infant if only adult pads are available?
When adult AED pads are the only option for an infant or small child, use anterior-posterior placement: one pad on the front of the chest (sternum) and one pad on the back between the shoulder blades. The pads must not touch or overlap. This placement ensures the electrical current passes effectively through the heart.
What happens immediately after a defibrillation shock in pediatric OSCE?
Immediately after delivering a defibrillation shock, resume CPR right away — do not pause to check the rhythm or pulse. Continue CPR for 2 full minutes before reassessing. Pausing prematurely is a common sequencing error in OSCE stations.
What are the critical errors in the pediatric CPR OSCE station?
The two most commonly flagged critical errors are: (1) using the wrong compression-to-ventilation ratio for the number of rescuers in the scenario, and (2) incorrect AED pad placement — particularly allowing pads to overlap or using anterior-only positioning on a small child or infant. Both are explicitly marked on the OSCE assessment sheet.
If You’re Looking for More Updates Like This – Explore:
Pediatric CPR OSCE Step by Step 2026 | Latest Pediatric CPR Algorithm 2026 | Pediatric OSCE Scenarios CPR | Pediatric Resuscitation Protocol Updates 2026
Get in touch:
 Website: www.nzsc.ac.nz
Website: www.nzsc.ac.nz Instagram: @nzsc_skillsconnect
Instagram: @nzsc_skillsconnect Facebook: New Zealand Skills Connect
Facebook: New Zealand Skills Connect WhatsApp: +64 22 903 2915
WhatsApp: +64 22 903 2915 Email: info@nzsc.ac.nz
Email: info@nzsc.ac.nz
Leave a Reply